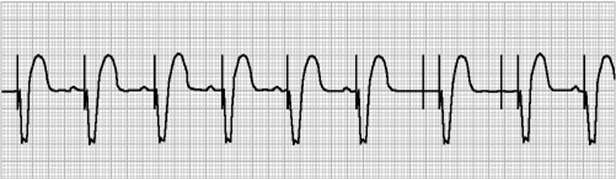
50. Choice B is the correct answer. There is ST elevation in leads II, III, and avF not ST depression or T wave inversion consistent with an inferior wall STEMI. This is not a normal EKG and there is no right bundle branch block on this EKG.
Wednesday, December 25, 2013
Question 50
50. Please interpret the EKG below:

A. Inferior Ischemia
B. Inferior STEMI
C. Normal EKG
D. Right Bundle Branch Block

A. Inferior Ischemia
B. Inferior STEMI
C. Normal EKG
D. Right Bundle Branch Block
Answer 49
49. Choice D is the correct answer. There is complete AV dissociation. Typical of third degree blocks the P waves and QRS complexes march out independently with calipers. Second degree AV block type I has lengthened PR interval that drops, where as the type II has a normal PR interval that the QRS complex just drops.
Question 49
49. Please interpret the EKG listed below:

A. Junctional Rhythm
B. Second Degree AV Block Type I
C. Second Degree AV Block Type II
D. Third Degree AV Block
A. Junctional Rhythm
B. Second Degree AV Block Type I
C. Second Degree AV Block Type II
D. Third Degree AV Block
Answer 48
48. Choice B is the correct answer. There is diffuse ST elevation throughout most of the leads of the EKG which is typical of Pericarditis. This is not a normal EKG. There is ST elevation in the inferior leads so there is no evidence of ischemia.
Question 48
48. Please interpret the EKG listed below:

A. Normal EKG
B. Pericarditis
C. Ventricular Tachycardia
D. Inferior Ischemia

A. Normal EKG
B. Pericarditis
C. Ventricular Tachycardia
D. Inferior Ischemia
Answer 47
47. Choice B is the correct answer. This is denoted by the R and R' wave seen in leads V1 and V2. If this was in lead V5 and V6 a left bundle branch should be considered. This is not a premature ventricular contraction.
Question 47
47. Please interpret the EKG listed below:

A. Left Bundle Branch Block
B. Right Bundle Branch Block
C. Premature Ventricular Contractions
D. Normal EKG
A. Left Bundle Branch Block
B. Right Bundle Branch Block
C. Premature Ventricular Contractions
D. Normal EKG
Answer 46
46. Choice C is the correct answer. There is a pacer spike occurring before the QRS complex. With a atrial pace maker there is a spike before the P wave if present. Dual chamber pacers have two pacer spikes on the EKG strip occurring before the QRS complex.
Question 46
46. Please interpret the EKG listed below:

A. Dual Chamber Pacer
B. Bundle Branch Block
C. Ventricular Pacer
D. Atrial Pacer
A. Dual Chamber Pacer
B. Bundle Branch Block
C. Ventricular Pacer
D. Atrial Pacer
Answer 45
45. Choice B is the correct answer. When the intrinsic rate is over 150, it needs to be determined if it a narrow complex tachycardia. If so, we can say that the pacemaker is coming from outside of the ventricles so we refer to it as supraventricular tachycardia (Paroxysmal atrial and junctional tachycardia). A-Fib with RVR is an irregular rhythm and has a rate over 100. Ventricular tachycardia is a wide complex tachycardia.
Question 45
45. Please interpret the EKG strip listed below:

A. Sinus Tachycardia
B. Supraventricular Tachycardia
C. Ventricular Tachycardia
D. Atrial Fibrillation with rapid ventricular response.

A. Sinus Tachycardia
B. Supraventricular Tachycardia
C. Ventricular Tachycardia
D. Atrial Fibrillation with rapid ventricular response.
Answer 44
44. Choice C is the correct answer. There are two pacer spikes occurring towards the end of the EKG strips. Some pacer are only demand pacers and will capture when needed. This is why there is two pacer spikes. If it is an atrial pacer the spikes will occur before there P wave. If it is a ventricular pacer the pacer spike will occur before the QRS complex.
Question 44
44. Please interpret the EKG listed below:

A. Atrial Pacemaker
B. Ventricular Pacemaker
C. Transient Dual Chamber Pacemaker
D. Atrial Hypertrophy
Answer 43
43. Choice B is the correct answer. The rate is less than 60 and is sinus so this defines sinus bradycardia. The intrinsic rate from the SA node is 60-100. Rates greater than 100 are referred to as sinus tachycardia. Junction rhythm will have intrinsic rates of 40-60 and have inverted P waves occurring before, during, or immediately after the QRS complex.
Question 43
43. Please interpret the EKG strip below. Ventricular rate is 52.

A. Normal Sinus Rhythm
B. Sinus Bradycardia
C. Sinus Tachycardia
D. Junctional Rhythm
A. Normal Sinus Rhythm
B. Sinus Bradycardia
C. Sinus Tachycardia
D. Junctional Rhythm
Answer 42
42. Choice B is the correct answer. Second Degree Type 2 AV Block has a normal PR interval and drops QRS complex. Second Degree Type I AV Block has a prolonged PR interval and drops a QRS complex. With First Degree AV Block there is just a prolonged PR interval. With a third degree AV block there is complete AV dissociation.
Question 42
42. Please interpret the EKG strip below:

A. Second Degree Type 1 AV Block
B. Second Degree Type 2 AV Block
C. First Degree AV Block
D. Third Degree AV Block
A. Second Degree Type 1 AV Block
B. Second Degree Type 2 AV Block
C. First Degree AV Block
D. Third Degree AV Block
Answer 41
41. Choice C is the correct answer. EKG changes associated with a pulmonary embolus are as follows: Lead I large S wave, Lead II ST depression, Lead III a Q wave with an inverted T wave. There is typically T wave inversion in leads V1-V4. There may also be a right bundle branch block present. Pericarditis would typically have diffuse ST elevation. Hyperkalemia will have peaked T waves and hypercalcemia causes the QT interval to be shortened.
Question 41
41. What is a potential diagnosis for the EKG listed below?

A. Pericarditis
B. Hyperkalemia
C. Pulmonary Embolus
D. Hypercalcemia

A. Pericarditis
B. Hyperkalemia
C. Pulmonary Embolus
D. Hypercalcemia
Subscribe to:
Comments (Atom)